The patient is a 70 year old male who presented with pain in the lateral side of his right wrist after accidentally striking the ground instead of the ball during a round of golf. He also reported an inability to grip his clubs for the remainder of the round and has a slight "pins and needles" feeling in his little finger. He is retired, and golf is his main hobby.
X-rays showed a wrist possible fracture but were inconclusive. A CT scan has shown a displaced hook of hamate facture. Although being eligible for surgery, and despite desiring to return to golf as soon as possible, the patient has rejected it, citing fear of the operation. Orthotic intervention is required in its stead.
The hamate is a carpal bone on the medial side in the distal row of the wrist with articulations with the 4th and 5th metacarpals, capitate and triquetrum. Its hook, or hamulus, is a prominence projecting anteriorly from the hamate (Marieb & Hoehn, 2009). It is an attachment point the flexor retinaculum and two of the muscles grouped in the hypothenar eminence, namely flexor digiti minimi brevis (FDMB) and oppenens digiti minimi. In some cases the FDMB is not present; the third hypothenar muscle, adductor digiti minimi, is larger in compensation in this case. Flexor carpi ulnaris, a wrist flexor originating in the forearm also attaches to the hook (Marieb & Hoehn, 2009). Additionally, numerous ligamentous attachments of the wrist are found at the hook. The hook forms the medial border of the carpal tunnel and lateral border of the ulnar canal, through which the ulnar nerve, artery and vein pass though (Bishop & Beckenbaugh, 1988; Briones & Aldridge III, 2010; Marieb & Hoehn, 2009).
Hook of hamate fracture will present with pain over the hypothenar eminence, and may become painful if pressure is applied to dorso-ulnar aspect of the hand (Gittlen, 1984). Fracture of the hook of hamate can lead to compression of the ulnar canal, either directly from bony fragments applying pressure to the nerve or indirectly from fracture associated bruising and swelling. Some variation may occur where the ulnar nerve bifurcates around the hamulus before reuniting on the distal side (Briones & Aldridge III, 2010). The ulnar nerve’s positioning leaves it vulnerable to damage from hook of hamate fracture. In the ulnar canal the nerve separates into the deep branch, supplying the muscles of the 4th and 5th digits, and the superficial branch that provides sensory innervation of the C8 dermatome (Marieb & Hoehn, 2009). Depending of the location of nerve compression neuropathy symptoms differ. Pressure applied to only the deep branch can cause minor clawing of the ring and little finger, reduced grip strength, pinch strength, and abduction of the 4th and 5th digits. This presentation is defined as fixed metacarpophalangeal joint hyperextension and interphalangeal joint flexion and caused by unopposed action of the respective antagonist muscles. Reduced grip strength, pinch strength, and abduction of the 4th and 5th digits is also likely to be present (Bishop & Beckenbaugh, 1988). Other intrinsic hand muscles supplied by the ulnar nerve, such as the lumbricals and interossei, are less likely to suffer weakness or paralysis because they are dually innervated by the median nerve (Marieb & Hoehn, 2009). Only considerable nerve damage would cause full claw hand presentation. Pressure applied to the superficial branch leads to sensory symptoms such as pain and paresthesia in the medial side of the 4th digit, the entire 5th digit, and the ulnar side of the volar and dorsal aspects of the hand (Bishop & Beckenbaugh, 1988; Egawa & Asai, 1983). If pressure is applied proximal to the bifurcation of the nerve, both motor and sensory symptoms would be present.
Hook of hamate fracture has 3 categories of mechanism of injury. Direct trauma to the hamulus is most often seen in baseball players, where the force of a swing is transferred directly to the hook, causing fracture (Lee, 2009; . Analogous mechanisms are seen in golfers that strike the ground instead of the ball, and players of racquet sports (Lee, 2009). Falling on an outstretched hand is a far less common mechanism of direct trauma injury. Stress fractures of the hook are seen in players of the same sports. This is thought to be caused by overuse of their swinging action (Bachoura, Wroblewski, Jacoby, Osterman & Culp, 2013; Scheufler, Andresen, Radmer, Erdmann, Exner & Germann, 2005). Indirect trauma from force applied to other parts of the wrist can cause stressful pulling on carpal ligaments leading to avulsion fracture of the hook.
Hook of hamate fractures account for 2% of carpal fractures, although it’s true incidence is unknown because of the difficulty of diagnosis (Briones & Aldridge III, 2010; Gittlen, 1984) . It is often mistaken for other injuries, commonly wrist sprain or tendonitis. It generally cannot be visualised with routine coronal and saggital X-rays (Andresen, Radmer, Scheufler, Adam & Bogusch, 2006; Egawa & Asai, 1983). Oblique x-rays are more likely to show the fracture. A CT scan is the most useful imaging technique for identifying hamulus fracture, although it is useful to acquire images of both hands to rule out congenital abnormality (Andresen et al., 2006). An MRI scan is also useful for determining whether associated nerve and soft tissue damage is present (Briones & Aldridge III, 2010).
Typically orthotic treatment is done by casting the wrist. There is a lack of literature concerning the use of other orthoses, especially in adults. Thermoplastic devices have the ability to provide the same immobilization properties while offering distinct advantages in hygiene and practicality. A volar orthosis is the usual prescription for hook of hamate fracture (Boyd, Benjamin & Asplund, 2009; Rizzone & Gregory, 2013). Depending on the design of a thermoplastic orthosis a patient may be able to remove the device and as a result compliance issues are a factor is choice of conservative treatment. Semi circumferential orthoses are better able to accommodate the swelling that is often present in patients with hamulus fracture than traditional casting (Boyd et al., 2009; Rizzone & Gregory, 2013). Durability is a concern in prescribing orthotics, and with good care a thermoplastic device will outlast a plaster cast but not a fiberglass cast. A further advantage of thermoplastic orthoses is they are cheaper than casting (von Keyserlingk, Boutis, Willan, Hopkins & Goeree, 2011). There is inconsistency in the literature regarding the extent of immobilization. One study reported immobilization of the wrist and 4th and 5th digits to the proximal interphalangeal joints, presumably reasoning that the complex articulations of the carpal bones and ligaments are placed under strain by digital movement (Egawa & Asai, 1983). Others leave the fingers unsplinted while most are non-specific, except to specify short arm casting (Boyd et al., 2009; Rizzone & Gregory, 2013). The most recent evidence points to leaving the digits unsplinted. Any wrist immobilisation orthosis should be applied with the wrist in a functional position ranging from neutral to 20 degrees of extension. The distal trim line must be placed to allow full elbow range of motion. Should surgery have been the method of treatment used for hamulus fracture, the wrist will require splinting or casting for a period of two to three weeks (Briones & Aldridge III, 2010). This does not alter the design or procedure of orthotic management.
Surgery is the preferred method of treatment of hook of hamate fracture. Either open reduction internal fixation (ORIF) or removal of the hamulus can be performed. Both operations give very good prospects for full recovery. Excision of the bone fragment is the more common procedure due to its relative simplicity and excellent prospects for recovery. ORIF of the hook of hamate is regarded as a technical procedure for minimal, if any, benefit over excision (Briones & Aldridge III, 2010). Removal of the hook eliminates the risk of post-treatment complications, usually non-union of the fracture and secondary nerve, artery and soft tissue damage that may be present in ORIF and orthotic treatment. Excision does remove the attachment point of a significant amount of ligamentous and muscular tissue which may prevent a return to a patient’s pre-injury level of grip strength; in practice, however, fewer patients are asymptomatic upon follow up of excision than ORIF. ORIF purports to preserve grip strength, but carries the risk of non-union and higher rates of continuing fracture symptoms post-treatment. However, this risk is much lower than external immobilization of the wrist. Rates of non-union in casting are unacceptably high (ranging from 50-90% in some studies (Scheufler et al., 2005) although the literature may paint an inaccurate picture of orthotic management’s efficacy. Typically hamulus fracture is not diagnosed immediately after the occurrence of the injury when immobilization therapy is at its most effective (De Schrijver & De Smet, 2001). Studies of acute phase hook of hamate fracture treated conservatively show acceptable rates of non-union and associated complications (Whalen, Bishop & Linscheid, 1992). It can be inferred that the timing of diagnosis is key in effective orthotic treatment of hook of hamate fracture. Surgical treatment is not reliant on quick diagnosis. Excision of the hook shows excellent results regardless of the time since the injury, and ORIF compares favourably (Carrol & Lakin, 1993). In most cases surgical treatment facilitates a return to activity with three months and patients are entirely asymptomatic . Overall, recovery from orthotic treatment tends to be inferior to surgical treatment, however good results can be achieved (Ge et al., 2010). A further advantage of surgical intervention is the ability to perform nerve release in the carpel or ulnar tunnel release if the patient requires it (Bachoura et al., 2013).
Treatment of the patient’s hamulus fracture involved two methods.
As a temporary measure, a plaster of paris slab cast was designed to promote fracture healing by immobilising the wrist until a more permanent device could be manufactured. Specifically, wrist flexion and extension and radial and ulnar deviation are restricted. Immobilisation also aims to relieve pain caused by the fracture. The initial plaster slab covered the forearm from an inch distal from the elbow joint to the distal palmar crease, with an opening for the thumb following the border of the thenar eminence. Its trim lines are intended to give the patient full range of motion at the elbow and metacarpophalangeal joints, as well as the carpometacarpal joint of the thumb. With the wrist casted in a slightly extended position, the slab provides as much functional ability as possible. The cast was slightly more than 50% circumferential, with its open side at the dorsal aspect. The semicircumferential design also aids in allowing for fluctuating volume in the injured area. It was held in place by wrapping non-compression bandages over the cast with the aim of holding the cast in place while still allowing for volume fluctuations.
Once swelling has subsided a secondary, and more permanent, low temperature thermoplastic device can be manufactured. Its design is much the same as the plaster of paris slab cast. Its design is also semicircumferential, applied with the wrist in slight extension and with trim lines not impinging on the range of motion of any joints other than the wrist and leaving the thumb completely mobile. The devices’ aim is the same as the plaster slab, while improving the hygiene, practicality and durability of orthotic intervention. Rather than using bandages, straps applied as proximally and distally as possible reduce pressure on the forearm, wrist and hand, while another placed over the wrist prevents wrist extension.
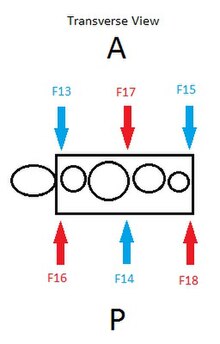
The low-temperature thermoplastic device is designed to sit on the volar aspect of the forearm, wrist and hand covering about 50̥ percent of the circumference. As such, no bony prominences need to be allowed for in the design. Trimlines are located an inch from the elbow crease, around the thenar eminence, and at the distal palmar crease. Strap placement is guided by the red forces of the force diagrams, while the thermoplastic forces are indicated by the blue arrows. Velcro straps attach to velcro hooks placed on the device, with the exception of the distal strap, which attaches directly to the thermoplastic at the radial side using a heat gun.
Have the patient place their pronated hand and forearm on a sheet of kitchen cloth. The fingers should be in their normal position and thumb should be abducted. Trace around the hand and forearm. Mark the distal palmar crease, MTP and IP joint of the thumb, as well as the position of the wrist joint (fig 2).
Draw the pattern of the orthosis on the same piece of cloth. Trim lines should be the distal palmar crease, an inch distal to the cubital fossa and between 1-2 inches of margin beyond the outline of the forearm to ensure semi-circumferential coverage. Elbow movement should not be affected by this device. The centre of the thumb hole should be in line with the midline of the index finger and and, perpendicular to this, the thumb. It should be large enough to allow the thenar eminence to fit through and not impinge thumb movement.̈
Cut out the pattern and fit to the patient. Make adjustments to the size of the plan as necessary.
2D Plan
Cut out pattern
Test fit on patient
Test fit on patient
If the size and position of the trim lines is correct transfer the design to low temperature thermoplastic.
Heat the thermoplastic in water in a frypan. The frypan should be at medium heat. Allow it to soften and become malleable.
Once soft, cut out the thumb hole, ensuring it is of adequate size. The plastic likely will begin to harden at this point. Place it back in the frypan to soften the material.
Patient positioning is important for ease of moulding the thermoplastic to their wrist and forearm. The patient should be seated, with their elbow resting on a surface (table, armrest etc.) and their hand raised. The srist should be in slight extension. The wrist should be in a neutral position to allow ease of access to the volar and dorsal aspects. The digits should be relaxed.
Remove the thermoplastic from the frypan, remove any water from the surface by placing it on a towel momentarily, then apply directly to the volar aspect of the wrist, hand and forearm. Make sure the thermoplastic does not impinge the thumb. Roll back the edges of the trimlines at the distal palmar crease and the thumb hole to ensure the plastic does not dig in to the skin. Make sure the thermoplastic covers the volar aspect of the limb and is at least semi-circumferential. The material will stretch while heated; use this property to ensure appropriate coverage. Ensure that the material does not self adhere. If it does, simply return it to the frypan. The thermoplastic will return to its original two-dimensional shape.
Once positioning of the thermoplastic is achieved, allow it to cool in place.
Transfer to low-temp thermoplastic
Heat plastic in frypan
Cut thumb hole
Apply to patient, mould plastic
Distal trim lines
When cool, briefly dip the proximal end of the device into the frypan and flare the edge to ensure comfort and skin integrity.
Using a heat gun, heat the adhesive side of velcro hooks and their intended placement site on the volar aspect of the device. This should be as proximal and distal as possible to reduce the pressure applied by the device to the limb. The third velcro hook should be place over the wrist.
With the orthosis fitted to the patient, the straps should be fitted. The should be long enough to be circumferential, but with minimal overhang. The two proximal straps should attach only to the velcro hooks (ie. they are removable). The distal strap should cover only the dorsal aspect of the hand. It should attach to the velcro hooks on medial side. On the lateral aspect of the orthosis it should be attached directly to the thermoplastic using the same method as for the velcro hooks. The distal strap should not be able to be removed from the orthosis.
Fit to the patient and adjust the straps as necessary.
The patient reports pain in the medial side of his right wrist and also reported an inability to grip his clubs for the remainder of the round and has a slight "pins and needles" feeling in his little finger.
X-rays showed a wrist possible fracture but were inconclusive. A CT scan has shown a displaced hook of hamate fracture. He was unable to grip objects as firmly as previously and lost resistive ROM. His ability to play golf was impaired.
The orthosis is therefore designed to immobilize the wrist to allow for healing of the fracture.
http://youtu.be/vaNgVYa5_kM
Outcome measures can be a useful part of clinical assessment. They are important for evaluating the effectiveness of a given intervention, and, as a result, for potentially acquiring funding for the prescribed splint. Their quantifiable nature gives outcome measures testing a high level of reliability compared to inter-rater subjective assessment. Testing functional ability specific to the injury site is crucial for determining the effectiveness of an orthotic intervention.
The QuickDASH (Disabilities of the Arm, Shoulder, and Hand) upper limb assessment gives a time-efficient guide to the functional ability of the patient. This questionnaire has good validity as a standalone test (Kennedy et al., 2013). Its results have been shown to be comparable to the more comprehensive DASH quiz (Gummesson, Ward & Atroshi, 2006). Its optional sport/performing arts module increases its relevance to the patient, given his desire to return to regular golf.
A higher score indicates a higher level of disability, ranging from 0 to 100. Prior to provision of the orthosis the patient scored 45, including the sport module. Clinical testing revealed a flexion/extension, radial/ulnar deviation, ROM grade of 4. However, the patient could only progress through his ROM against very light resistance. Upon increased resistive force he was unable to progress through the ROM of the contralateral wrist. His grip strength was also impaired compared to the contralateral wrist. His pronation and supination was unaffected and reports light pins and needles.
After the prescribed treatment period the patient was retested. On this occasion he scored 21 on the QuickDASH. Clinical testing showed improvement in each movement of ROM; although his score remained at 4, the level of resistance he was able to progress through was higher. His grip strength was also significantly improved. Self reports of lingering minor pins and needles continued beyond orthotic treatment.
The patient’s post-intervention results showed improvement, which indicates healing. However, the presence of pins and needles may mean the ulnar nerve remains impinged. As with the initial diagnosis of this type of fracture, determining the true cause requires extensive medical imaging.
Andresen, R., Radmer, S., Scheufler, O., Adam, C. & Bogusch G. (2006). Optimization of conventional X-ray images for the detection of hook of hamate fractures. Rontgenpraxis, 56(2), 59-65. doi:10.1016/j.rontge.2005.08.001
Bachoura, A., Wroblewski, A., Jacoby, S.M., Osterman, A.L., & Culp, R.W. (2013). Hook of hamate fractures in competitive baseball players. Hand, 8, 302-307. doi:10.1007/s11552-013-9527-4
Bishop, A.T., & Beckenbaugh, R.D. (1988). Fracture of the hamate hook. The Journal of Hand Surgery, 13a(1), 135-139.
Boyd, A.S., Benjamin, H.J., & Asplund, C. (2009). Splints and casts: Indications and methods. American Family Physician, 80(5), 491-499.
Carrol, R.E., & Lakin, J.F. (1993). Fracture of the hook of hamate: Acute treatment. The Journal of Trauma, 34(6), 803-805.
Egawa M., & Asai, T. (1983). Fracture of the hook of hamate: Report of six cases and the suitablility of computerized tomography. The Journal of Hand Surgery, 8(4), 393-398.
De Schrijver, F., & De Smet, L. (2001). Fracture of the hook of hamate, often diagnosed as “wrist sprain”. The Journal of Emergency Medicine, 20(1), 47-51.
Ge, X., Lufai, D., Wei, Z., Yankun, S., & Guanglei, T. (2010). Clinical classification and treatment strategy of hamate hook fracture. Journal of Huazhong University of Science and Technology [Medical Sciences], 30(6), 762-766. doi:10.1007/s11596-010-0654-7
Gummesson, C., Ward, M. M., & Atroshi, I. (2006). The shortened disabilities of the arm, shoulder and hand questionnaire (QuickDASH): validity and reliability based on responses within the full-length DASH. BMC Musculoskeletal Disorders, 7(1), 44.
doi:10.1186/1471-2474-7-44
Kennedy, C. A., Beaton, D. E., Smith, P., van Eerd, D., Tang, K., Inrig, T., ... Couban, R. (2013). Measurement properties of the QuickDASH (Disabilities of the Arm, Shoulder and Hand) outcome measure and cross-cultural adaptations of the QuickDASH: a systematic review. Quality of Life Research, 22(9), 2509-2547.
von Keyserlingk, C., Boutis, K., Willan, A. R., Hopkins, R. B., & Goeree, R. (2011). Cost-effectiveness analysis of cast versus splint in children with acceptably angulated wrist fractures. International Journal of Technology Assessment in Health Care, 27(2), 101-7. doi:http://dx.doi.org/10.1017/S0266462311000067
Lee, A.D. (2009). Golf-related stress fractures: A structured review of the literature. Journal of the Canadian Chiropractic Association, 53(4), 291-299.
Marieb, E.N., & Hoehn, K. (2009). Human anatomy and physiology (8th ed.). San Francisco, CA. Pearson Benjamin Cummings.
Rizzone, K., & Gregory, A. (2013). Using casts, splints, and braces in the emergency department. Clinical Pediatric Emergency Medicine, 14(4), 340-348.
Scheufler, O., Andresen, R., Radmer, S., Erdmann, D., Exner, K., & Germann, G. (2005). Hook of hamate fractures: Critical evaluation of different therapeutic procedures. Plastic & Reconstructive Surgery, 115(2), 488-497. doi:10.1097/01.PRS.0000149480.25248.20
Whalen, J.L., Bishop, A.T., & Linscheid, R.L. (1992). Nonoperative treatment of acute hamate hook fractures. The Journal of Hand Surgery, 17(3), 507-511. doi:10.1016/0363-5023(92)90363-T
Databases used included La Trobe Library, Scopus, CINAHL, Medline. Search terms included hamate fracture, hamulus fracture, ortho*, management, brace, splint,