ICD-10 Coding/Certain Infectious and Parasitic Diseases
This lesson introduces ICD-10-CM Certain Infectious and Parasitic Diseases.
Objectives and Skills
editObjectives and skills for this lesson include:
edit- Correctly apply ICD-10-CM coding guidelines for accurate selection and sequencing of diagnosis codes commonly used to describe infectious and parasitic diseases.
- Apply ICD-10-PCS coding guidelines for accurate selection of procedure codes commonly used to diagnose and treat infectious and parasitic diseases.
- Explain the differences between bacteremia, septicemia, SIRS, sepsis, and septic shock, and how to code these conditions.
- Explain how to code HIV testing, diagnosis, and treatment.
- Assess strategies to identify key solutions to code infections and parasitic diseases
- Create a writing assignment
Guidelines and Coding Examples
edit-
 Symptoms of AIDS
Symptoms of AIDS

Code only confirmed cases of HIV infection/illness. This is an exception to the hospital inpatient guideline Section II, H. In this context, “confirmation” does not require documentation of positive serology or culture for HIV; the provider’s diagnostic statement that the patient is HIV positive, or has an HIV-related illness is sufficient.-Serologic Testing for HIV Infection
2) Selection and sequencing of HIV Codes:
editIf a patient is admitted for an HIV-related condition, the principal diagnosis should be B20, Human immunodeficiency virus [HIV] disease followed by additional diagnosis codes for all reported HIV-related conditions.
If a patient with HIV disease is admitted for an unrelated condition (such as a traumatic injury), the code for the unrelated condition (e.g., the nature of injury code) should be the principal diagnosis. Other diagnoses would be B20 followed by additional diagnosis codes for all reported HIV-related conditions.
Whether the patient is newly diagnosed or has had previous admissions/encounters for HIV conditions is irrelevant to the sequencing decision
Z21, Asymptomatic human immunodeficiency virus[6] [HIV] infection status, is to be applied when the patient without any documentation of symptoms is listed as being “HIV positive,” “known HIV,” “HIV test positive,” or similar terminology. Do not use this code if the term “AIDS” is used or if the patient is treated for any HIV-related illness or is described as having any condition(s) resulting from his/her HIV positive status; use B20 in these cases.
Patients with inconclusive HIV serology, but no definitive diagnosis or manifestations of the illness, may be assigned code R75, Inconclusive laboratory evidence of human immunodeficiency virus [HIV].
Patients with any known prior diagnosis of an HIV-related illness should be coded to B20. Once a patient has developed an HIV-related illness, the patient should always be assigned code B20 on every subsequent admission/encounter. Patients previously diagnosed with any HIV illness (B20) should never be assigned to R75 or Z21, Asymptomatic human immunodeficiency virus [HIV] infection status.
During pregnancy, childbirth or the puerperium, a patient admitted (or presenting for a health care encounter) because of an HIV-related illness[8] should receive a principal diagnosis code of O98.7-, Human immunodeficiency [HIV] disease complicating pregnancy, childbirth and the puerperium, followed by B20 and the code(s) for the HIV-related illness(es). Codes from Chapter 15 always take sequencing priority. Patients with asymptomatic HIV infection status admitted (or presenting for a health care encounter) during pregnancy, childbirth, or the puerperium should receive codes of O98.7- and Z21.
If a patient is being seen to determine his/her HIV status, use code Z11.4, Encounter for screening for human immunodeficiency virus [HIV]. Use additional codes for any associated high risk behavior. If a patient with signs or symptoms is being seen for HIV testing, code the signs and symptoms. An additional counseling code Z71.7, Human immunodeficiency virus [HIV] counseling, may be used if counseling is provided during the encounter for the test. When a patient returns to be informed of his/her HIV test results and the test result is negative, use code Z71.7, Human immunodeficiency virus [HIV] counseling. If the results are positive, see previous guidelines and assign codes as appropriate.
Certain infections are classified in chapters other than Chapter 1 and no organism is identified as part of the infection code. In these instances, it is necessary to use an additional code from Chapter 1 to identify the organism. A code from category B95, Streptococcus, Staphylococcus, and Enterococcus as the cause of diseases classified to other chapters, B96, Other bacterial agents as the cause of diseases classified to other chapters, or B97, Viral agents as the cause of diseases classified to other chapters, is to be used as an additional code to identify the organism. An instructional note will be found at the infection code advising that an additional organism code is required.
Many bacterial infections are resistant to current antibiotics[10]. It is necessary to identify all infections documented as antibiotic resistant. Assign a code from category Z16, Resistance to antimicrobial drugs, following the infection code only if the infection code does not identify drug resistance.
-
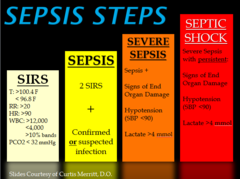 Sepsis Steps
Sepsis Steps

For a diagnosis of sepsis, assign the appropriate code for the underlying systemic infection. If the type of infection or causal organism is not further specified, assign code A41.9, Sepsis, unspecified organism. A code from subcategory R65.2, Severe sepsis, should not be assigned unless severe sepsis or an associated acute organ dysfunction is documented.
- (i) Negative or inconclusive blood cultures and sepsis
- Negative or inconclusive blood cultures do not preclude a diagnosis of sepsis in patients with clinical evidence of the condition; however, the provider should be queried.
- (ii) Urosepsis
- The term urosepsis is a nonspecific term. It is not to be considered synonymous with sepsis. It has no default code in the Alphabetic Index. Should a provider use this term, he/she must be queried for clarification.
- (iii) Sepsis with organ dysfunction[12]
- If a patient has sepsis and associated acute organ dysfunction[12] or multiple organ dysfunction (MOD), follow the instructions for coding severe sepsis.
- (iv) Acute organ dysfunction that is not clearly associated with the sepsis
- If a patient has sepsis and an acute organ dysfunction, but the medical record documentation indicates that the acute organ dysfunction is related to a medical condition other than the sepsis, do not assign a code from subcategory R65.2, Severe sepsis. An acute organ dysfunction must be associated with the sepsis in order to assign the severe sepsis code. If the documentation is not clear as to whether an acute organ dysfunction is related to the sepsis or another medical condition, query the provider.
The coding of severe sepsis requires a minimum of 2 codes: first a code for the underlying systemic infection, followed by a code from subcategory R65.2, Severe sepsis. If the causal organism is not documented, assign code A41.9, Sepsis, unspecified organism, for the infection. Additional code(s) for the associated acute organ dysfunction are also required. Due to the complex nature of severe sepsis, some cases may require querying the provider prior to assignment of the codes.
Septic shock[12] generally refers to circulatory failure associated with severe sepsis, and therefore, it represents a type of acute organ dysfunction.
For cases of septic shock, the code for the systemic infection should be sequenced first, followed by code R65.21, Severe sepsis with septic shock or code T81.12, Post-procedural septic shock. Any additional codes for the other acute organ dysfunctions should also be assigned. As noted in the sequencing instructions in the Tabular List, the code for septic shock cannot be assigned as a principal diagnosis.
If severe sepsis is present on admission, and meets the definition of principal diagnosis, the underlying systemic infection should be assigned as principal diagnosis followed by the appropriate code from subcategory R65.2 as required by the sequencing rules in the Tabular List. A code from subcategory R65.2 can never be assigned as a principal diagnosis.
When severe sepsis develops during an encounter (it was not present on admission), the underlying systemic infection and the appropriate code from subcategory R65.2 should be assigned as secondary diagnoses.
Severe sepsis may be present on admission, but the diagnosis may not be confirmed until sometime after admission. If the documentation is not clear whether severe sepsis was present on admission, the provider should be queried.
If the reason for admission is both sepsis or severe sepsis and a localized infection, such as pneumonia or cellulitis, a code(s) for the underlying systemic infection should be assigned first and the code for the localized infection should be assigned as a secondary diagnosis. If the patient has severe sepsis, a code from subcategory R65.2 should also be assigned as a secondary diagnosis. If the patient is admitted with a localized infection, such as pneumonia, and sepsis/severe sepsis doesn’t develop until after admission, the localized infection should be assigned first, followed by the appropriate sepsis/severe sepsis codes.
5) Sepsis due to a post-procedural infection
editAs with all post-procedural complications, code assignment is based on the provider’s documentation of the relationship between the infection and the procedure.
For infections following a procedure, a code from T81.40, to T81.43 Infection following a procedure, or a code from O86.00 to O86.03, Infection of obstetric surgical wound, that identifies the site of the infection should be coded first, if known. Assign an additional code for sepsis following a procedure (T81.44) or sepsis following an obstetrical procedure (O86.04). Use an additional code to identify the infectious agent. If the patient has severe sepsis, the appropriate code from subcategory R65.2 should also be assigned with the additional code(s) for any acute organ dysfunction. For infections following infusion, transfusion, therapeutic injection, or immunization, a code from subcategory T80.2, Infections following infusion, transfusion, and therapeutic injection, or code T88.0-, Infection following immunization, should be coded first, followed by the code for the specific infection. If the patient has severe sepsis, the appropriate code from subcategory R65.2 should also be assigned, with the additional codes(s) for any acute organ dysfunction.
If a post-procedural infection has resulted in post-procedural septic shock, assign the codes indicated above for sepsis due to a post-procedural infection, followed by code T81.12-, Post-procedural septic shock. Do not assign code R65.21, Severe sepsis with septic shock. Additional code(s) should be assigned for any acute organ dysfunction.
In some cases a noninfectious process (condition), such as trauma, may lead to an infection which can result in sepsis or severe sepsis. If sepsis or severe sepsis is documented as associated with a noninfectious condition, such as a burn or serious injury, and this condition meets the definition for principal diagnosis, the code for the noninfectious condition should be sequenced first, followed by the code for the resulting infection. If severe sepsis is present, a code from subcategory R65.2 should also be assigned with any associated organ dysfunction(s) codes. It is not necessary to assign a code from subcategory R65.1, Systemic inflammatory response syndrome (SIRS) of non-infectious origin, for these cases. If the infection meets the definition of principal diagnosis, it should be sequenced before the non-infectious condition. When both the associated non-infectious condition and the infection meet the definition of principal diagnosis, either may be assigned as principal diagnosis. Only one code from category R65, Symptoms and signs specifically associated with systemic inflammation and infection, should be assigned. Therefore, when a non-infectious condition leads to an infection resulting in severe sepsis, assign the appropriate code from subcategory R65.2, Severe sepsis. Do not additionally assign a code from subcategory R65.1, Systemic inflammatory response syndrome (SIRS) of noninfectious origin. See Section I.C.18. SIRS due to non-infectious process
See Section I.C.15. Sepsis and septic shock complicating abortion, pregnancy, childbirth and the puerperium
See Section I.C.16. f. Bacterial sepsis of Newborn[12]
Resisting Infections[15]Methicillin Resistant Staphylococcus aureus (MRSA)[16] Conditions
edit-
 MRSA
MRSA
_Bacteria_(6830393029).jpg)
Selection and Sequencing of MRSA codes
editWhen a patient is diagnosed with an infection that is due to methicillin resistant Staphylococcus aureus (MRSA), and that infection has a combination code that includes the causal organism (e.g., sepsis, pneumonia) assign the appropriate combination code for the condition (e.g., code A41.02, Sepsis due to Methicillin resistant Staphylococcus aureus or code J15.212, Pneumonia due to Methicillin resistant Staphylococcus aureus). Do not assign code B95.62, Methicillin resistant Staphylococcus aureus infection as the cause of diseases classified elsewhere, as an additional code, because the combination code includes the type of infection and the MRSA organism. Do not assign a code from subcategory Z16.11, Resistance to penicillins, as an additional diagnosis. See Section C.1. for instructions on coding and sequencing of sepsis and severe sepsis.
When there is documentation of a current infection (e.g., wound infection, stitch abscess, urinary tract infection) due to MRSA, and that infection does not have a combination code that includes the causal organism, assign the appropriate code to identify the condition along with code B95.62, Methicillin resistant Staphylococcus aureus infection as the cause of diseases classified elsewhere for the MRSA infection. Do not assign a code from subcategory Z16.11, Resistance to penicillins.
The condition or state of being colonized or carrying MSSA or MRSA is called colonization or carriage, while an individual person is described as being colonized or being a carrier. Colonization means that MSSA or MSRA is present on or in the body without necessarily causing illness. A positive MRSA colonization test might be documented by the provider as “MRSA screen positive” or “MRSA nasal swab positive”. Assign code Z22.322, Carrier or suspected carrier of Methicillin resistant Staphylococcus aureus, for patients documented as having MRSA colonization. Assign code Z22.321, Carrier or suspected carrier of Methicillin susceptible Staphylococcus aureus, for patient documented as having MSSA colonization. Colonization is not necessarily indicative of a disease process or as the cause of a specific condition the patient may have unless documented as such by the provider.

If a patient is documented as having both MRSA colonization and infection during a hospital admission, code Z22.322, Carrier or suspected carrier of Methicillin resistant Staphylococcus aureus, and a code for the MRSA infection may both be assigned.
Code only a confirmed diagnosis of Zika virus (A92.5, Zika virus disease) as documented by the provider. This is an exception to the hospital inpatient guideline Section II, H. In this context, “confirmation” does not require documentation of the type of test performed; the physician’s diagnostic statement that the condition is confirmed is sufficient. This code should be assigned regardless of the stated mode of transmission.
If the provider documents "suspected", "possible" or "probable" Zika, do not assign code A92.5. Assign a code(s) explaining the reason for encounter (such as fever, rash, or joint pain) or Z20.821, Contact with and (suspected) exposure to Zika virus.
Learning Resources
editCoding Guidelines[15]:
https://www.cms.gov/Medicare/Coding/ICD10/Downloads/2019-ICD10-Coding-Guidelines-.pdf
Differences between Bacteremia and Septicemia:
https://microbiologyinfo.com/differences-between-bacteremia-and-septicemia/[18]
CDC website - Sepsis:
https://www.cdc.gov/sepsis/what-is-sepsis.html[19]
AIDS Disease[20] :
https://www.britannica.com/science/AIDS
AIDS Facts[21]:
https://www.britannica.com/science/AIDS/media/10414/120213
HIV and AIDS Resources[22]:
https://www.cms.gov/Outreach-and-Education/Outreach/HIVAIDSRes/index.html
Tuberculosis[23]:
https://www.cdc.gov/tb/publications/pamphlets/tbandhiv_eng.htm
Gram-positive vs. Gram-negative Bacteria
Activities
editSepsis Quiz:
http://hitnots.com/sepsis-quiz-trial-being-tested/[24]
Severe Sepsis Quiz:
http://hitnots.com/severe-sepsis-quiz-being-tested/[25]
Septic Shock Quiz:
http://hitnots.com/septic-shock-quiz-being-tested/[26]
Watch the following video and answer the question: When to use Z codes vs B codes when coding HIV cases?
https://www.youtube.com/watch?v=qPKCii4zYUA[27]
Coding Sepsis, Severe Sepsis & Septic shock Quiz:
http://hitnots.com/coding-sepsis-severe-sepsis-septic-shock-quiz-being-tested/[28]
Create a PPT:
After completing assigned reading and watching assigned videos create a short PPT presentation focusing on key differences between Bacteremia, Septicemia, Sepsis, Severe Sepsis, SIRS and Septic Shock in the order from lowest to greatest severity.
Gram-Negative vs Gram-Positive Bacterial Infections:
After visiting the following websites write a short summary about Gram-Negative vs Gram-Positive Bacterial Infections.
Be sure to include causes, risk factors, diagnosis, symptoms and treatments.
- https://www.diffen.com/difference/Gram-negative_Bacteria_vs_Gram-positive_Bacteria[30]
- Table: http://www.cfsph.iastate.edu/Disinfection/Assets/BacteriaGroupReviewTable.pdf[31]
Coding Bootcamp:
After watching the Coding Bootcamp video from 2015, note if the assigned codes were correct and explain why or why not?
ICD-10-CM Coding Bootcamp: Infectious and Parasitic Diseases [32] https://www.youtube.com/watch?v=09NlIF2tBxM
West Nile Virus Activity:
Pretend you are an HIM Director and your task is to write a memo to your staff informing them about the West Nile Virus and appropriate codes. Be sure to include an example of a coding scenario. Please visit the following websites to gather your information. https://www.cdc.gov/westnile/index.html[33], https://icd.who.int/browse10/2016/en#/A92.3[34]
-
 West Nile Transmission Cycle
West Nile Transmission Cycle

Zika Virus Activity: Your assignment is to create an 8 question quiz about Zika Virus after visiting the Mayo-clinic website and reading ICD-10-CM guidelines. Questions should pertain to coding guidelines, as well as signs and symptoms of the disease. https://www.mayoclinic.org/diseases-conditions/zika-virus/expert-answers/zika-virus/faq-20178199[35]
-
 Symptoms of Microcephaly
Symptoms of Microcephaly

Tuberculosis[3]: After visiting http://bok.ahima.org/doc?oid=302589#.XI7_NRNKiqA[36] write a short paragraph summarizing how the new ICD-11th edition reflects changes with regards to Tuberculosis.
-
 Symptoms of Tuberculosis
Symptoms of Tuberculosis

Summary
editReview
edit- Diagnosis Guidelines and Code Scenarios (see Guidelines and Coding Examples)
- See Also: Wikipedia page referencing codes pertaining to infectious and parasitic diseases
Assessment
edit- See Activities, Key terms and Learning Resources.
- Assessment Quiz
Key Terms
edit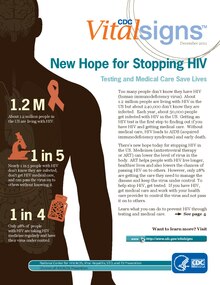
Bacteremia - presence of bacteria in the bloodstream after trauma or an infection.
HIV[37] - Human Immunodeficiency Virus
Nosocomial Infections[3]:Secondary infections that are contracted as a result of a medical treatment or develop during hospitalization.
Septicemia - a systemic disease associated with pathological microorganisms or toxins in the bloodstream.
Sepsis - is the body’s extreme response to an infection. It is a life-threatening medical emergency.
Sepsis happens when an infection you already have —in your skin, lungs, urinary tract, or somewhere else—triggers a chain reaction throughout your body.
Without timely treatment, sepsis can rapidly lead to tissue damage, organ failure, and death[38]
SIRS - systemic inflammatory response syndrome: a systemic response to infection or trauma with such symptoms as fever and tachycardia
Septic Shock - circulatory failure associated with severe sepsis.
Toxic Shock Syndrome[3] - A48.3 - Caused by bacterial infection.
- Symptoms include high fever of sudden onset, vomiting, watery diarrhea, myalgia, followed by hypotension and sometimes shock.
- Originally reported exclusively in menstruating women using high - absorbency tampons
- Code responsible organism (B95-B96)
See Also
edit
Wikipedia
editICD-10-Chapter 1: Certain infectious and parasitic diseases at Wikipedia.[39]
References
edit- ↑ "Login". Dropbox. Retrieved 2019-04-24.
- ↑ What is HIV and AIDS?, retrieved 2019-03-28
- ↑ 3.0 3.1 3.2 3.3 3.4 author., Leon-Chisen, Nelly. ICD-10-CM and ICD-10-PCS coding handbook, without answers 2018. ISBN 9781556484339. OCLC 975367466. http://worldcat.org/oclc/975367466.
- ↑ Diagnosing HIV - Concepts and tests, retrieved 2019-03-28
- ↑ "Asymptomatic HIV infection: MedlinePlus Medical Encyclopedia". medlineplus.gov. Retrieved 2019-03-28.
- ↑ "Asymptomatic HIV infection: MedlinePlus Medical Encyclopedia". medlineplus.gov. Retrieved 2019-04-24.
- ↑ "Pregnancy and HIV". The Well Project. 2018-07-10. Retrieved 2019-03-28.
- ↑ "Pregnancy and HIV". The Well Project. 2018-07-10. Retrieved 2019-04-24.
- ↑ "What is antibiotic resistance?". Khan Academy. Retrieved 2019-03-28.
- ↑ "What is antibiotic resistance?". Khan Academy. Retrieved 2019-04-24.
- ↑ iMedicalSchool (2012-04-01), Medical School - Sepsis in 5 Minutes, retrieved 2019-03-28
- ↑ 12.0 12.1 12.2 12.3 Sepsis: Systemic inflammatory response syndrome (SIRS) to multiple organ dysfunction syndrome (MODS), retrieved 2019-03-28
- ↑ Septic shock - pathophysiology and symptoms, retrieved 2019-03-28
- ↑ "Neonatal sepsis: MedlinePlus Medical Encyclopedia". medlineplus.gov. Retrieved 2019-03-28.
- ↑ 15.0 15.1 "Acrobat Accessibility Report" (PDF). www.cms.gov. Retrieved 2019-03-17.
- ↑ "General Information | MRSA | CDC". www.cdc.gov. 2019-02-25. Retrieved 2019-03-28.
- ↑ "Zika virus". www.who.int. Retrieved 2019-03-28.
- ↑ Aryal, Sagar. "Differences Between Bacteremia and Septicemia". Microbiology Info.com. Retrieved 2019-03-11.
- ↑ CDC (2019-01-15). "Sepsis is a medical emergency. Time matters". Centers for Disease Control and Prevention. Retrieved 2019-02-16.
- ↑ "AIDS | Definition, Diagnosis, Treatment, & Facts". Encyclopedia Britannica. Retrieved 2019-03-17.
- ↑ "AIDS | Definition, Diagnosis, Treatment, & Facts". Encyclopedia Britannica. Retrieved 2019-03-17.
- ↑ Medicare, Centers for; Baltimore, Medicaid Services 7500 Security Boulevard; Usa, Md21244 (2017-06-27). "Overview". www.cms.gov. Retrieved 2019-03-27.
- ↑ "The Connection between TB and HIV | Pamphlets, Brochures, Booklets| Publications & Products | TB | CDC". www.cdc.gov. 2018-12-11. Retrieved 2019-03-27.
- ↑ "Sepsis Quiz". Health Information Technology Notifications | HITNOTS. 2016-06-06. Retrieved 2019-02-16.
- ↑ "Severe Sepsis Quiz". Health Information Technology Notifications | HITNOTS. 2016-06-06. Retrieved 2019-02-16.
- ↑ "Septic Shock Quiz". Health Information Technology Notifications | HITNOTS. 2016-06-06. Retrieved 2019-02-16.
- ↑ MedicalCodingCert (2016-04-18), HIV ICD-10-CM Codes - When to Use Z Code vs. B Code, retrieved 2019-03-25
- ↑ "Coding Sepsis, Severe Sepsis & Septic Shock Quiz". Health Information Technology Notifications | HITNOTS. 2016-06-06. Retrieved 2019-02-16.
- ↑ "Gram-negative Bacterial Infection | Winchester Hospital". www.winchesterhospital.org. Retrieved 2019-03-18.
- ↑ "Gram-positive vs Gram-negative Bacteria - Difference and Comparison | Diffen". www.diffen.com. Retrieved 2019-04-01.
- ↑ http://www.cfsph.iastate.edu Bacterial Group Review Table
- ↑ VantagePoint HealthCare Advisors (2016-01-12), ICD-10-CM BootCamp: Certain Infectious and Parasitic Diseases, retrieved 2019-02-16
- ↑ "West Nile virus | West Nile Virus | CDC". www.cdc.gov. 2018-12-10. Retrieved 2019-02-19.
- ↑ "ICD-10 Version:2016". icd.who.int. Retrieved 2019-04-01.
- ↑ "What is the Zika virus, and should I be worried?". Mayo Clinic. Retrieved 2019-02-19.
- ↑ Palkie, Brooke; Kerr, Katie MA (2018-10-01). "WHO Releases ICD-11 Preview". WHO Releases ICD-11 Preview / AHIMA, American Health Information Management Association. PMID 302589. http://bok.ahima.org/doc?oid=302589.
- ↑ "Treatment Adherence Tips for HIV Patients | HIV Answers®". www.hivanswers.com. Retrieved 2019-03-28.
- ↑ CDC (2019-01-15). "Sepsis is a medical emergency. Time matters". Centers for Disease Control and Prevention. Retrieved 2019-02-16.
- ↑ "ICD-10 Chapter I: Certain infectious and parasitic diseases". Wikipedia. 2018-08-15. https://en.wikipedia.org/w/index.php?title=ICD-10_Chapter_I:_Certain_infectious_and_parasitic_diseases&oldid=855046522.